

Loading...
25 June 2026 / Report
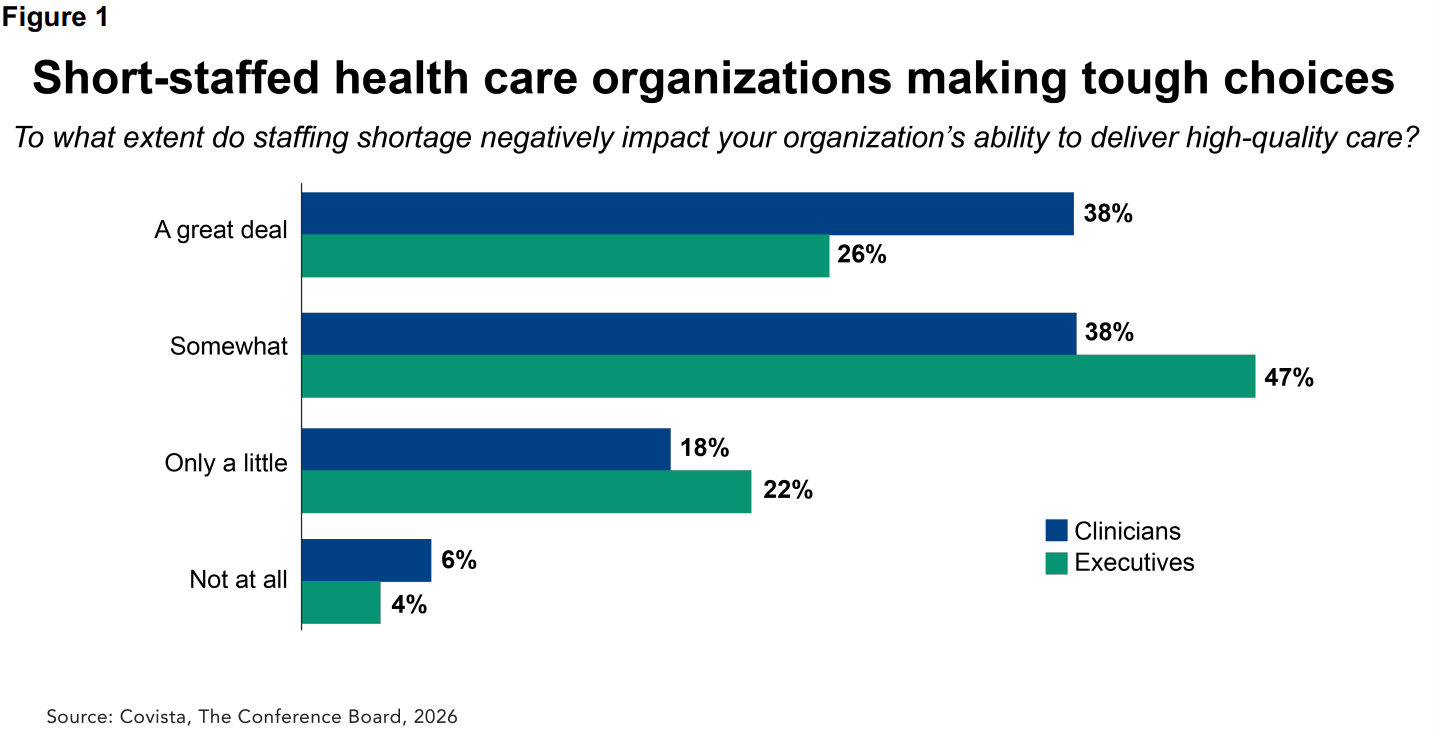
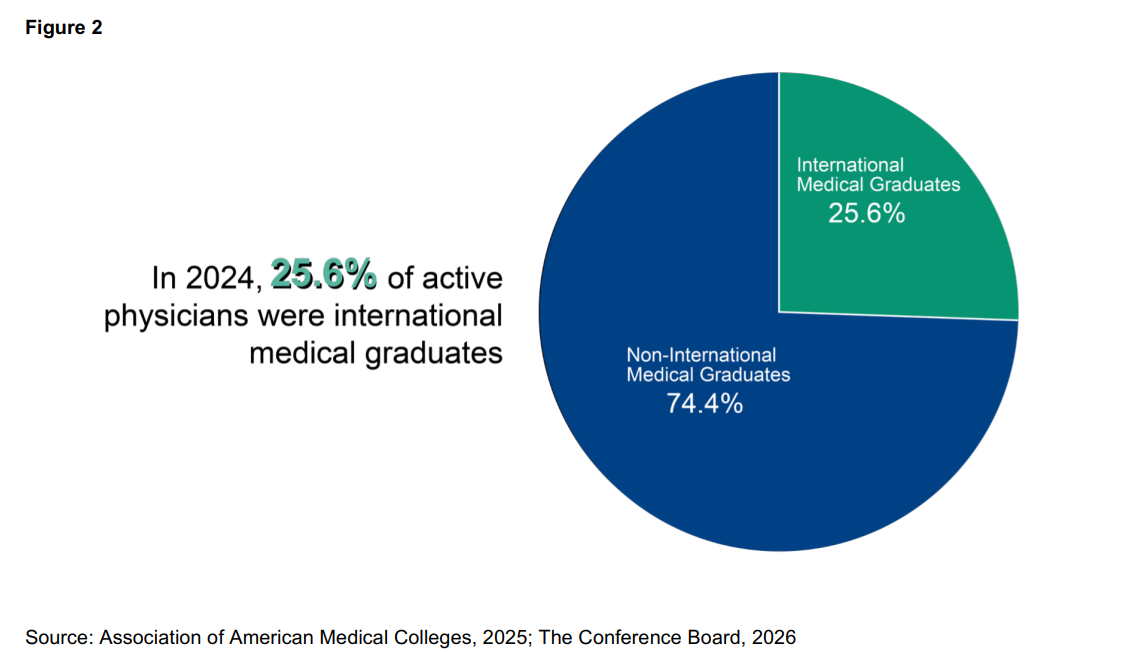
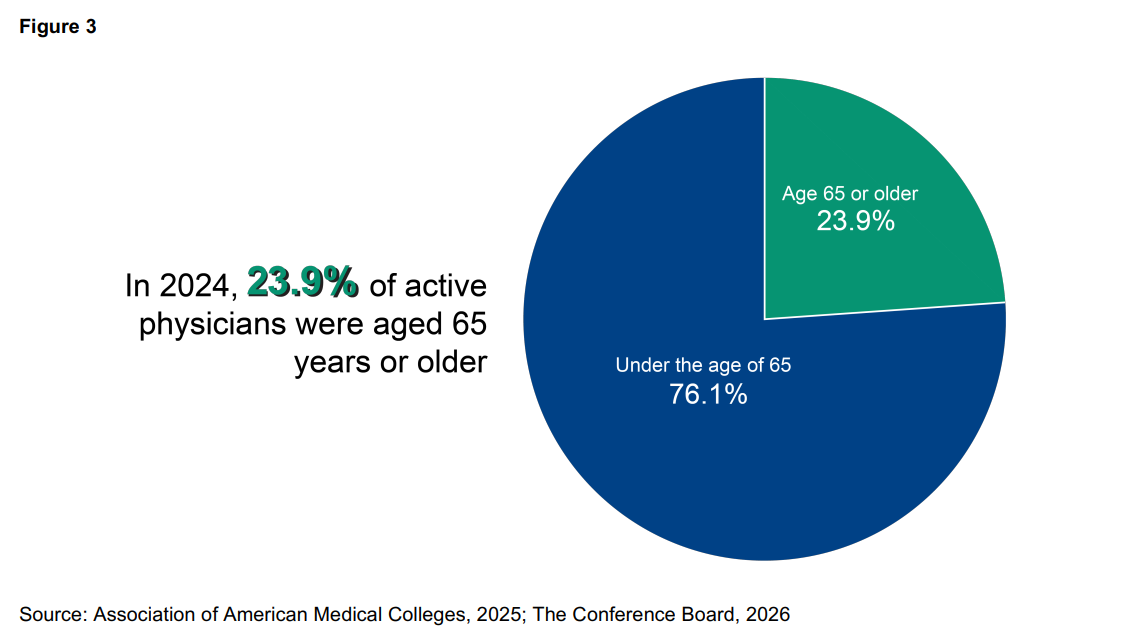
Despite the extraordinary advances of science in the last 50 years, the US health care system can be only as good as the workforce that delivers it. In the US, there are more than 700,000 job openings in the health care sector each month—and only 306,000 unemployed workers available to fill them.1 The health care crisis is real, but there are actionable solutions. This Solutions Brief outlines policy steps to help solve workforce gaps: expand pathways into the workforce, improve retention and job quality, promote team-based and preventive care, and deploy technology in innovative ways that expand effective capacity while preserving trust, safety, and quality. The US spends more on health care than any comparable country yet often does not achieve top results on key measures of health system performance and outcomes.2 One step to ending this disparate result is enabling a vibrant, well-trained, clinically prepared, and effective health care workforce. The health care workforce gap now directly affects a broad swath of factors, including access, outcomes, and systemic performance. Rising demand for care, driven by aging, chronic disease, and greater care complexity, are colliding with constrained training capacity, uneven distribution, administrative burden, and postpandemic attrition. Expanding head count alone will not solve the problem. Workforce shortages reflect weaknesses across the full system: entry pathways, training infrastructure, retention, care delivery design, and the policy environment that shapes how talent is financed and deployed. Limited faculty, preceptors, clinical placements, and community-based training capacity continue to restrict the number of workers who can move efficiently from interest into practice, especially within high-need communities. Retention and job quality are now central workforce issues. Burnout, clerical overload, weak supervision, staffing instability, and poor work design reduce effective supply and make shortages harder to reverse. Factors including payment, regulation, and technology will increasingly determine whether the system can modernize successfully. Reimbursement rules, licensure barriers, immigration frictions, and poorly implemented digital tools can all impede workforce capacity, while improved alignment across these areas can strengthen access and workforce stability. FOREWORD Steve Beard, Chairman and CEO, Covista The health care workforce crisis is not coming. It is here. More than 700,000 health care job vacancies every single month. Half of health care executives have already cut patient capacity—reduced hours, closed beds, fewer visits—not as a future contingency, but as a present reality. The clinicians left standing are stretched past what any system should ask of them. According to the Covista Care Capacity Monitor, 76% of them say staffing shortages are compromising their ability to deliver high-quality care. Not eventually. Now. Behind those numbers are patients who wait longer, travel farther, and in too many cases simply go without. The health care workforce crisis is not an operational problem confined to hospital boardrooms. It is a public health crisis felt in waiting rooms and emergency departments, in rural towns where the nearest specialist is hours away, and in communities where a shortage of home health aides means an elderly parent cannot age with dignity. Every unfilled position is a person who needed care and did not receive it. What makes this moment different—and what the Addressing US Health Care Workforce Shortages report captures with particular clarity—is that the approaches we have relied upon are not working. Higher pay is not closing the gap. Recruiting bonuses are not closing the gap. Competing harder for the same limited pool of workers will never close the gap. The math is structural: for every unemployed health care worker in America, employers post more than two new openings every month. We are not facing a distribution problem that better incentives can solve. We are facing a supply problem that only structural change can address. Technology will play a role. Artificial intelligence, automation, and care model redesign can make the workforce we have more efficient and effective—extending the reach of every nurse, physician, and allied health professional. But technology cannot replace the workforce we do not have. Tools that improve productivity are not a substitute for workers. The problem is supply and it requires a fundamentally different response. That response will not come from any single sector acting alone. The health care workforce gap will require education, health care, business, policy, and communities to work together in ways they have not before—aligning training capacity with employer need, removing the regulatory and financial barriers that slow new clinicians from entering practice, accelerating pathways for internationally trained clinicians, and building the kind of durable workforce infrastructure this moment demands. These are not simple asks. They require sustained coordination across organizations that have historically operated in parallel rather than in partnership. But the cost of continued fragmentation—measured in patients, in clinicians, and in communities—is no longer acceptable. The good news is that the solutions exist. Across the country, health systems, education institutions, state agencies, and employers are piloting innovative approaches that work—grow-your-own programs that recruit from the communities they serve, education and employer partnership models that compress time to practice without sacrificing quality, and regulatory reforms that let skilled workers practice at the top of their training. What has been missing is not innovation. It is the will and the coordination to act on these approaches at scale. This report is offered in that spirit. It names the scope of the crisis clearly, examines what the evidence says about what works, and lays out a practical agenda for action. The health care workforce this country needs is achievable. But only if we build it together, deliberately, and starting now. Actions for policymakers (Federal, State, and local government) include: Expand and diversify pathways into health care careers through earlier exposure to them, clearer school-to-career routes, scholarships, and nontraditional training models. Northwell School of Health Sciences in New York City is an excellent model to encourage health care careers in local communities, particularly among underserved populations. Expand training infrastructure, including faculty, preceptors, clinical placements, community-based teaching capacity, and stronger educator-provider partnerships. Reinforce primary care as the foundation of access to health care by addressing disincentives that steer clinicians away from primary care and align clinical training capacity with patient and population needs. Support recruitment and retention in rural and underserved communities by aligning training, placement, and financial support with local workforce need. Reform payment systems so reimbursement better supports prevention, value through outcomes, primary care, care coordination, and multidisciplinary team-based care rather than service volume alone and reduce avoidable paperwork that diverts time from patients. Address geographic shortages, particularly in rural and underserved communities, and reduce barriers that limit workforce deployment by expanding telehealth and licensure portability, and using immigration pathways, including credential bridges, for clinicians trained abroad. Actions for business include: Build stronger pipelines through employer-educator partnerships that expand apprenticeships, earn-and-learn models, and clear career ladders into high-need roles. An example of this is the work Covista is doing with health care systems like SSM Health, whose Aspiring Nurse Program trains students within the facilities where they work, creating direct pathways to employment and delivering practice-ready nurses into high-need roles. Terumo Blood and Cell Technologies similarly supports stronger pipelines by partnering with Colorado colleges, technical programs, and nursing educators to introduce students and early-career nurses to apheresis, building awareness of a critical and specialized field enabling the future of biotechnology. Build the health care workforce across the full career journey, as demonstrated by the focus of Covista Open Doors , a multiyear impact commitment to build and sustain the health care workforce, investing across each stage of the health care career continuum through career exploration partnerships, emergency financial support for students, and mental health and well-being programs for practicing clinicians. Treat retention as a workforce strategy by supporting professional development and advancement, workplace safety, team-based care, reducing administrative burdens, and better job design. Scale team-based care so professionals can work at the top of their license, expanding effective capacity and improving patient experience and outcomes. Deploy technology and human-complementary AI to improve clinical decision making, streamline administration, and improve job quality, supported by strong governance and privacy rules. Expanding the productivity of the clinical workforce will expand the capacity of the clinical workforce. A March 2026 policy summit on the health care workforce, hosted by CED in partnership with the Covista Foundation and also sponsored by Northwell Health and Terumo Blood and Cell Technologies, highlighted structural drivers of shortages and solutions that point the way forward. 3 The summit advanced CED’s work on strengthening the US health care workforce and driving innovation through business-led collaboration. Effective responses must address not only the number of workers entering the field, but also the strength of pathways into practice; training and retention once workers arrive; and the financing, regulatory, and technological conditions that determine whether health systems can deploy talent effectively. CED was honored to host this summit and looks forward to remaining strongly engaged in this issue so important for our economy and for Americans’ health. The US health care workforce faces a widening gap between the care Americans need and desire and the system’s capacity to deliver it. As demand accelerates and training too often remains constrained, the state of the health care workforce has become not only an issue for the health care sector, but an issue of the Nation’s competitiveness and economic resilience. In today’s US health care workforce, which exceeds 18 million, 4 shortages increasingly shape labor market performance, employer costs, and the resilience of a sector that has become one of the country’s largest sources of job growth; the New York Times accurately describes the health care workforce as the “lifeblood of the labor market.” 5 An aging population, rising chronic disease burden, and growing care complexity increase service intensity, while workforce supply remains limited by training bottlenecks, uneven distribution, administrative burdens, and retirements and attrition. The result is reduced access, higher operating costs for providers, and mounting pressure on providers, employers, and payers. Addressing shortages requires more than expanding headcount; it requires modernizing how care is delivered. As Covista Chairman and CEO Steve Beard comments: “This is a patient care crisis. Half of health care leaders have already cut beds and reduced patient capacity. That’s happening now, not someday.” 6 To take only one example, the Covista Care Capacity Monitor states that 85% of health care leaders in rural communities cannot find the workforce they need to respond to community demands for care. Even as demands for the clinical workforce grow, the traditional pathways into these roles have not grown, and too many qualified students cannot find places in medical or nursing school. Persistent workforce challenges threaten America’s health, economic competitiveness, and fiscal sustainability. Health care continues to account for a disproportionate share of US job growth, underscoring that demand pressures are structural rather than cyclical. At the same time, rapid technological change is reshaping both clinical and administrative work, offering the potential to amplify scarce clinician time and deploy technology in ways that can measurably improve productivity, job quality, and access to high-quality care. Whether these tools strengthen the workforce will depend upon implementation, governance, and care redesign. The issue is urgent and essential. As Michael Dowling, CEO Emeritus of Northwell Health, asks, for a health care business to thrive, “what is more important than the asset that walks in every morning and walks out at night?” The most recent Federal projections point to a sustained gap between health care needs and the workforce available to meet them. The Health Resources and Services Administration’s (HRSA) National Center for Health Workforce Analysis projects substantial physician shortages by 2038 across most specialties, with especially important implications for “front door” access where patients first engage the health system.7 HRSA projects similar shortages in nursing, with larger gaps outside metropolitan areas, as well as shortfalls across several allied health, oral health, and behavioral (mental) health professions. HRSA also notes that projections based on current utilization likely understate need because they do not capture unmet demand. Nonmetropolitan areas, defined as those not having “an urban core of 50,000 or more people,”8 will bear the brunt of these gaps. By 2038, HRSA projects that physician supply in nonmetro areas will meet only 42% of projected demand, compared with a 5% shortage in metro areas. The same pattern appears in specific disciplines, including a 39% primary care physician shortfall and a 46% OB-GYN shortfall in nonmetro areas. As of December 2025, approximately 92 million people lived in a primary care Health Professional Shortage Area (HPSA), 64 million in a dental HPSA, and 137 million in a mental health HPSA. These figures underscore that workforce constraints are not hypothetical risks to access, but present structural realities. The Covista Care Capacity Monitor found that 50% of executive leaders say shortages have reduced their capacity to serve patients, while 76% of clinicians and 73% of executives said staffing shortages compromise their ability to deliver high-quality care.9 The survey also identified a widening pipeline mismatch, with more than 700,000 health care job postings per month versus about 306,000 unemployed health care workers available to fill them, and even sharper constraints in rural and less urban communities. The report also provided labor market analysis state-by-state showing the clear mismatch between health care needs and both geographic and specialty shortages. Demand-side drivers The Medicare population is steadily both increasing and aging and, with it, demand is rising for more intensive and complex care.10 This shift affects not only the volume of care required, but also the importance of workplace models suited to delivering care in a variety of settings: outpatient, home-based, behavioral health, and the broader community as well as traditional settings. An important aspect of this change is rising demand for long-term services as more older adults live with disability, chronic illness, and functional limitations that require ongoing assistance. In 2022, 18.5% of people ages 65 and older reported a disability. Among Medicare beneficiaries ages 65 and older, 37% in 2021 reported limitations in activities of daily living or instrumental activities of daily living or were living in a long-term care facility.11 All of this places growing pressure on the long-term services and supports workforce, including both clinical and nonclinical caregiving roles. Because much of this care depends on direct support and caregiving roles that sit outside the traditional physician-centered workforce frame, long-term services and support (LTSS) is an indispensable aspect of addressing health care workforce shortages. Causes of shortages derive from the entire course of the workforce cycle. The workforce challenge reflects not only rising demand, but also a persistent mismatch between the system’s need for workers and its ability to build, support, and transition people into health care careers. Vulnerabilities in the pipeline appear early. Many students receive too little exposure to the range of health care careers and their benefits, too little encouragement to pursue them, and too little practical support in navigating a path from school into work. These barriers can be especially acute for younger students, first-generation entrants, learners from underserved communities, and those who do not follow traditional academic routes into the profession. Attracting people to the profession is more difficult because of chronic underinvestment in STEM education to spark interest in and desire for health careers early in life and underinvestment in training programs, both in nursing and graduate medical education. Qualified students still struggle to access seats in medical, nursing, and other health professional programs even as employers face acute labor shortages. The problem is not simply a shortage of interest or talent. It is also a shortage of opportunities, training capacity, and structured pathways into practice.12 Formal training capacity is another major bottleneck. Faculty shortages, clinical placement limits, accreditation timelines, and uneven financing all slow the expansion of workforce supply. In practice, the binding constraint is often not interest in health careers, but the formal system’s limited ability to add seats, support teaching, and move trainees efficiently into practice.13 Taking the example of physicians, medical school enrollment reached 99,562 students in academic year 2024–2025,14 but physicians cannot enter independent practice without residency, and Medicare-funded Graduate Medical Education caps continue to constrain training capacity. The Government Accountability Office (GAO) found that in 2018, 70% of hospitals were over one or both Medicare-funded resident caps, indicating that hospitals can train more physicians than current payment limits support.15 National Resident Matching Program data likewise show continued pressure at the point of entry into residency. On the nursing side, constraints are even more explicit: The American Association of Colleges of Nursing (AACN) reports that nursing programs turned away 80,162 qualified applications in 2024 because of insufficient faculty, clinical sites, preceptors, classroom space, and budget.16 Within health care settings, shortages often reflect simple supply and demand: fewer providers and more people requiring care because of aging and care of chronic diseases, leading to greater strains on the system that in turn make careers in health care professions less attractive. Unrealistic patient expectations in an already-stressed system sometimes lead to episodes of violence against health care workers. As the perception of risk rises, the attractiveness of the profession and retention fall. Poorly designed electronic medical records systems increase administrative burdens and lead to burnout. More broadly, criticisms of science, public health, and academic freedom diminish the attractiveness of health care as a career; as one health care leader puts it, “progress moves at the speed of trust.”17 For providers, regulations from the Centers for Medicare and Medicaid Services (CMS) that intend to improve quality can conversely result in excessive administrative burdens of documenting services to ensure compliance. Inadequate reimbursement to hospitals can provide the perverse incentive to reduce staff, placing a greater burden on those who deliver care. Efforts by other payors to limit reimbursements (for instance, rules on preauthorization) can add administrative burdens. Dental care experiences similar shortages resulting from challenges in access, capacity, geography, reimbursement, licensure, scope of practice, and general operations. Similarly, because oral health is essential to good overall health, there is a strong business case for prevention in oral health as well, particularly for high-risk population for whom simple assessments can yield better outcomes while reducing systemic costs. Effective solutions must address not only the number of workers entering the field, but also the strength and diversity of the pathways that lead into practice; retention of workers and their job satisfaction; and the financing, regulatory, and technological conditions that determine whether health systems can deploy talent effectively. Expand and diversify workforce pathways Building the health care workforce of the future means responding to needs in the workforce.18 In turn, this means making pathways more visible earlier in students’ lives, exposing students earlier to the range of health care careers (including nursing, pharmacy, allied health, behavioral health, and roles such as community health workers, care coordinators, and home-based care professionals), the stability of these careers, and the value of a career built on serving others. Educators should make the prospect of careers in health care realistic and attainable for students, not least through expanded STEM education, which is the foundation. One example of employer-education partnership that widens and strengthen health care workforce pathways is the Northwell School of Health Sciences in Queens, which opened in September 2025 through a partnership among Northwell Health, New York City Public Schools, the Fund for New York City Public Schools, and Bloomberg Philanthropies.19 The school enrolled an inaugural class of approximately 240 students and, at full capacity, is expected to serve roughly 900 students annually. The school’s design reflects an effort to connect education more directly to workforce need: students are introduced to four career-focused pathways—pre-nursing, medical assisting, behavioral and mental health, and health care management—and may graduate with industry-recognized credentials and/or college credits, along with hands-on learning and mentorship tied to real care settings. This model suggests how earlier, more structured, and employer-connected pathways could help make health care careers more visible, attainable, and responsive to community and labor market needs. Apprenticeships also offer opportunities for a serious examination of health care careers and strong preparation for those who enter them. Beyond registered apprenticeships, which included 36,892 in the health care industry in 2025 (up 43% in five years), programs such as Washington State’s Health Care Apprenticeship Consortium, which includes partners from employers, unions, and the state, and is open to all health care employers serve as models for building what the Consortium describes as a “state-wide healthcare educational pathway through multiple apprenticeship opportunities, that is used by healthcare employers across the state and promotes accessibility, retention, and stability within the healthcare workforce.”20 At the tertiary level, this will also involve efforts to reduce the financial barriers that keep many qualified entrants from pursuing careers in health care. Reducing financial and structural barriers to entry must be part of any serious health workforce strategy. The burden is substantial, with 71% of medical school graduates in 2024 carrying education debt, and a median debt load of $205,000 among those with debt.21 Employer partnerships can generate additional and new, often nontraditional, pathways. Covista’s workforce initiatives aim at addressing these barriers directly. Last year, Chamberlain University and SSM Health launched the Aspiring Nurse Program, which combines tuition support, immersive clinical training within SSM Health facilities, and a pathway to employment across four states.22 Since then, applications for the program have jumped 117% in St. Louis and nearly 200% in Oklahoma City. Projected to produce more than 400 practice-ready nurses annually, the program illustrates how employer-education partnerships can expand access to training and help more qualified entrants pursue and complete health care career pathways. Lasting impact also requires sustained commitment. Covista offers a useful model for how workforce pathways can be widened and better aligned with employer demand across the full career journey. Through Covista Open Doors, the company frames workforce development not as a one-time intervention, but as sustained investment in career exploration, financial support, and worker well-being.23 This approach recognizes that workforce pathways often fail to respond to actual labor market need unless they are scaled intentionally and are built in partnership with the organizations that employ health care workers. By linking early exposure to health careers, support for persistence and completion, and stronger connections to employment, the model suggests how pathway strategies can become more durable, more connected to employers, and more responsive to workforce shortages over time. Similarly, Northwell Health invests in internal workforce development through its Center for Learning and Innovation, the health system’s corporate university, which provides continuous learning, leadership development, and role-specific training for employees. A 2017 quality report demonstrates the long-standing scale of its investment in workforce development as a sustained institutional priority: the Center delivered more than 260,700 hours of training to 58,014 employees, suggesting that in-house workforce development has been a sustained institutional priority rather than a recent initiative.24 Together, these efforts illustrate how employer-connected pathways can begin earlier, continue on the job, and help make health care careers more visible, attainable, and responsive to community and labor market needs. Health care careers generally require specialized training, yet structural challenges in training too often prevent interest in health care careers from achieving students’ dreams. In practice, bottlenecks often include shortages of faculty, clinical sites, classroom space, and clinical preceptors, as well as budget constraints. Solutions include financing the infrastructure that makes training possible for faculty, clinical placements, preceptors, and community-based teaching capacity, as well as expanding graduate medical education models that place residents in outpatient and underserved settings. HRSA’s Teaching Health Center Graduate Medical Education Program offers one example, supporting the training of physicians and dentists in community-based settings focused on rural and underserved communities. This model shows how workforce investments can better align training with access needs, primary care delivery, and community demand.25 University-based models point in the same direction. At the University of Wisconsin School of Medicine and Public Health, graduates of the Wisconsin Academy for Rural Medicine practice in rural Wisconsin at substantially higher rates than other graduates, suggesting that training pathways deliberately rooted in rural communities can improve workforce distribution as well as overall supply.26 Together, these models show how workforce investments can better align training with access needs, primary care delivery, and community demand. That is a useful reminder that workforce expansion depends not only on tuition or scholarships, but also on the less visible institutional capacity that allows these kinds of programs to operate and grow. Similarly, Thomas Jefferson University has long had a Physician Shortage Area Program. Launched in 1974, the program selectively admits medical students from rural areas who intend to practice in rural communities and then supports them through mentoring and rural clinical experiences during medical school. Graduates are 8.5-9.9 times more likely than their peers to enter rural family medicine, and long-term retention in rural family medicine remains above 70% after 20-25 years of practice.27 Once training is complete, transitions from training into employment are a critical moment in ensuring successful health care careers. Stronger handoffs from education into practice, clearer school-to-career routes, and closer coordination among educators, care delivery organizations, and employers ensure that workers enter the positions for which they have been trained. Policymakers and employers should therefore enable infrastructure for workforce expansion, including scholarships, faculty support, preceptor development, clinical placement capacity, and stronger educator-provider partnerships. Immigration policy directly affects workforce shortages because many health systems, including those in rural and other underserved communities, rely upon internationally trained health care workers as a meaningful share of their staffing pipeline. The American Hospital Association found that immigrant and noncitizen workers are overrepresented in the health care field overall, are more concentrated in high-demand roles, and contribute meaningfully to staffing in rural communities, where shortages are often most acute.30 Specifically, International Medical Graduates (IMGs) account for roughly one-quarter of active US physicians,31 and county-level evidence shows they continue to make a significant contribution in Medically Underserved Areas (MUAs) even as the number of US medical graduates has grown.32 Similarly, immigrants account for about 16.7% of all nurses,33 and hospitals have increasingly reported hiring foreign-educated RNs to help address vacancies. In the long-term care sector, immigrants make up more than 800,000 workers, or 28% of the direct care workforce overall; most are naturalized citizens, while roughly 300,000 are noncitizens.34 Given that reliance, even routine visa frictions, such as processing pauses, delays, or changes in fees, can impact staffing for providers that depend on internationally trained clinicians to cover in demand roles. Research on immigration policy and the health care workforce finds that easing restrictions on international medical graduates can increase physician supply in underserved areas without evidence of crowding out US-trained doctors. That directly affects care capacity in rural and underserved communities35 and points to several practical policy responses.36 First, the Federal government can help relieve workforce shortages by expanding and streamlining visa pathways for qualified medical workers. Second, the Conrad 30 waiver program remains an important mechanism for placing foreign-trained physicians in underserved communities and should be preserved and strengthened. Third, policymakers and employers should build credential-bridging pathways for foreign-trained health professionals by allowing them to enter the workforce in roles below the level they held in their home country and then permitting them to test up to the US equivalent of their foreign license. These sector-specific reforms would help providers fill workforce gaps more quickly while expanding access to care in rural and underserved communities and long-term care settings. As the general population ages, so does the workforce. To retain and bring back older health care workers, workplace design can help make staying in the workforce more attractive. Efforts to reduce administrative burdens and expand the use of technology—so long as older workers are trained in it—will have positive effects on retention. During the pandemic, independent workers were a critical source of supply and remain so in many locations. Though they are often deployed as lower-skilled independent contractors, training and upskilling these workers ensures they are used most effectively in the roles for which they are hired. This reinforces a virtuous cycle of training and practice, with educational institutions offering both brick-and- mortar and virtual training as the new norm, enabling independent workers to rise in their careers.37 Cleveland Clinic, for example, uses flexible scheduling and pro re nata (PRN) nursing options as retention tools, suggesting one practical way health systems can make continued workforce participation more feasible for experienced clinicians.38 Additionally, health care employers can work collaboratively with community colleges to ensure that their curricula prepare future workers not to merely pass a licensing exam, but to excel and advance in today’s health care system.39 Northwell Health’s Center for Learning and Innovation provides this support for workforce development through continuous learning, tuition reimbursement, and targeted training pathways in roles such as nurse assistant and allied health.40 Improve retention and job satisfaction Because training pathways are so long and require a great deal of investment, the health care sector must focus on retention to a greater degree than other sectors, and this focus yields correspondingly greater rewards. Retention depends upon more than compensation. Leadership visibility, strong onboarding, mentorship, workplace safety, and clear communication between leaders and frontline staff all shape both whether workers remain in the field and whether they feel able to do their jobs well. Wise and durable workforce strategies treat employees as a productive asset that requires sustained investment. Workforce resilience also depends upon trust. Leadership, supervision, and workplace culture should therefore be treated as core workforce infrastructure rather than as secondary management concerns. Workers are less likely to stay when clerical work spills into after-hours or when organizations rely on informal discretionary efforts rather than sustainable job design and team support. In an integrated literature review on intergenerational preferences within the workforce, Millennials expect “strong leadership, advancement opportunities, alignment of organizational and personal values, good coworker relationships, healthy work-life balance, recognition, and cutting-edge technology,” and concluded that they “have specific expectations for work, and they will leave if these go unmet.”41 This research does not speak only to preferences; it suggests that retention increasingly depends on whether care delivery systems are designed to support workers within the workday rather than depending on open-ended expectations of extra effort. The Agency for Healthcare Research and Quality’s Team Strategies and Tools to Enhance Performance and Patient Safety (TeamSTEPPS) program provides a structured framework for communication, team leadership, situation monitoring, and mutual support. This approach reinforces the policy case for retention strategies that invest in team-based work design, supervisory capacity, and stronger day-to-day care delivery systems rather than placing the burden of resilience on individual workers alone.42 Team-based care is a delivery model in which patient needs are addressed as coordinated efforts among multiple health care providers and across settings of care.43 As Antoinette Gawin, President and CEO of Terumo Blood and Cell Technologies, notes, there is a “huge opportunity to “look holistically across the system, organize around the patient, and develop a patient-centric model” for health care, at the same time “making it simpler and focusing on outcomes.” In team-based care, it is essential to ensure that all health care professionals are practicing at “the top of their license”—doing all things for which they were trained and licensed—while at the same time seeking to increase their scope of practice. In this way, team-based care can alleviate shortages both by making the health care professions more attractive (because people are practicing at the top of their licenses) and by providing greater and higher utilization of all health care practitioners. One benefit of well-implemented team-based care is alleviating stress on physicians.44 Physicians are autonomous decisionmakers, but providing them with leadership training to work in a team can help instill teamwork and reduce burnout. Education can also play a role here; medical schools can orient around team-based care and how physicians can operate in a team-based care system, engaging nurse practitioners, medical assistants, and mental health professionals as part of a team. Similarly, Gawin adds that freeing up time for clinicians gives them “time for active listening and displaying empathy in soft skills and bedside manner” which both leads to better health outcomes and gives health care workers an “anchor” in understanding why they entered health care professions: to care for people. Improving team support can make clinical work more sustainable and reduce reliance on extraordinary sacrifice as a substitute for sound operating design. Similarly, to improve workplace culture, “stay” interviews can foster connections between supervisors and employees and encourage a supportive environment.45 In today’s health care workplaces, with increased threats and actual violence against health care workers, workplace safety is also a workforce supply issue. Policymakers should be careful to determine where rules can inadvertently deter growth of team-based care. For instance, ambiguity over the Stark Law 46 prohibiting self-referral by physicians in Federal health programs can prevent strong collaboration of providers along an episode of care, including from providers that might be owned or controlled by a single provider group. Better cooperation could prevent missed opportunities on transition of care and outcomes. Reimbursement and licensure Payment design helps determine which workforce models the system can afford to sustain. In both Medicare fee-for-service and commercial coverage, primary care accounts for only a small share of total spending, suggesting that the financial base for prevention, continuity, and team-based workforce infrastructure remains thin.47 Fee-for-service also rewards billable encounters more readily than many of the activities on which a strained workforce increasingly depends, including care coordination, panel management, communication outside the visit, and other team-based functions that do not always generate separate reimbursement.48 It leads to rate disparity between primary and specialist care, which skews supply of physicians to specialties rather than to the frontlines of care, where providers can help diagnose and intervene in chronic conditions earlier. Payment reform should support the workforce models the system needs. This means reforming payment systems, including for private insurers, so that reimbursement supports modern patterns of care delivery. When health systems face very low operating margins, their space for innovation and workforce expansion is correspondingly reduced, highlighting the urgency of focusing on reimbursement in addressing health care shortages. When executed well, payment reform is also workforce reform. Reimbursement that undervalues nontraditional settings, multidisciplinary teams, and coordinated delivery can push organizations back toward fragmented models that are harder to staff and less resilient over time. More durable reforms will require payment approaches that reward prevention, care coordination, and person-centered team-based care rather than service volume alone. Growing research on comprehensive primary care payment argues that upfront, predictable payments are better suited than fee-for-service alone to support care coordination, staffing, and other practice capabilities essential to team-based care. This points toward payment models that give providers the stability to invest in prevention, relationships, and the infrastructure of longitudinal care rather than reimbursing only discrete services.49 For the post-acute sector, the largest problem is insufficient Medicare and Medicaid reimbursement, the primary source of revenue for so many of these providers. Absent greater pay, employees will leave for other sectors. Too often, regulatory barriers also limit the ability of the health care workforce to serve where it is needed. In the US system, states regulate the practice of medicine and regulation of health professions and differ in how clinicians can practice. For example, the National Conference of State Legislatures (NCSL) documents that nurse practitioner practice and prescription authority varies substantially by state, ranging from full independent authority to models requiring ongoing physician relationships.50 In our federal system, the solution is interstate licensure, to improve clinicians’ ability to practice across jurisdictions. In addition to the Interstate Medical Licensure Compact and Nurse Licensure Compact, the National Academy for State Health Policy similarly highlights state levers to strengthen access and expand team-based primary care, reinforcing the value of licensure policies that make workforce capacity more portable and responsive to both provider and patient needs.51 The Interstate Medical Licensure Compact Commission reports that nearly 50,000 physicians have used this pathway, and about 54% report intending to use their licenses to provide services in rural or underserved areas.52 Similarly, the Nurse Licensure Compact similarly expanded portability across participating jurisdictions, reaching 42 member jurisdictions by the end of fiscal year 2024.53 Licensure portability and scope-of-practice reform (for instance, greater treatment by Physicians’ Assistants and Nurse Practitioners) expands workforce capacity. For organizations that operate in multiple states, greater portability can help deploy workers more efficiently across settings and geographies, including in high-need communities.54 While licensure reform raises political challenges, it is one of the most practical solutions to remove frictions on cost and allocation of labor across the US health care system. Telehealth expansion is another practical workforce strategy, with particular benefits for rural and underserved communities and to serve the elderly. In 2023, CMS reported that telehealth expanded access for the more than 61 million Americans living in rural areas.55 Telehealth remains a vital part of care delivery: CMS reports that 6.73 million Medicare fee-for-service beneficiaries used a telehealth service in 2024, or 25% of eligible users.56 Continued reimbursement across state lines in Medicare and Medicaid and continued regulatory reform would help sustain those gains.57 Today’s new members of the health care workforce enter careers in which technology will define many aspects of care. More experienced health care workers face the challenge of learning new technologies and applying them to their workstreams. In the context of the health care workforce, it is best to think of technology as amplifying that workforce, enhancing its capacity to deliver better health care outcomes. For instance, technology works well in synthesizing content and fragmented data, including offering suggestions, to help clinicians make decisions. But technology is only useful when it provides the right data to the right clinician at the right time. Broadly speaking, beyond the benefits of new technologies to direct patient outcomes, technology works best when it helps expand effective workforce capacity to reduce administrative burden and redesign workflows so care teams can spend more time on patient-facing care. But technology also has a double role: Technology should be preventive (helping advance positive outcomes) and supportive (helping health care workers do their jobs better and more efficiently, reducing burnout and promoting retention.) All this permits clinicians to devote more time to exercising the judgment for which they were trained, communication, empathy, and direct care for patients. With the growth in the number of technology tools, including AI, attention is shifting to practical pathways through which technology and AI can amplify workforce capacity and clinical accuracy for better outcomes, including by improving education and training, easing administrative burdens, supporting care redesign, and expanding prevention and screening. Technology’s role in all these areas will only grow in the years ahead, with many impacts on the workforce. Education and training One clear application of technology is to enhance learning and training. Greater use of technology in educational, workplace, and other training settings can improve conditions for students—for instance, offering more flexible learning options that can reach nontraditional students and thus expand workforce pathways. As digital literacy too often remains an obstacle to effective deployment of technology, it is vital to develop curricula that ensure students are prepared to use technologies in the workplace. It also helps students understand what work in a contemporary, and often technology-driven, health care workplace is like. For today’s workforce, this may involve developing curricula for AI fluency. Covista is an example of this approach in practice, bringing education and technology together—working with partners to develop AI credentials that run alongside traditional clinical curricula and build the foundational skills health systems say they need most. It also means evaluating tools to understand better which expand workforce effectiveness and which tools inadvertently introduce more friction into the workplace. For the future workforce, continued STEM focus in schools makes health care careers seem more realistic and better prepares students for those careers. Reducing administrative burdens One promising use of technology focuses on reducing documentation and other administrative burdens that pull clinicians away from patients. The clearest opportunities involve repetitive nonclinical tasks such as electronic health record (EHR) documentation, inbox management, coding and billing support, prior authorization, scheduling, referral coordination, and routine patient communication. EHR design and usability also affect job quality and burnout risk. A multi-site quality improvement study across six health systems found that ambient AI scribes were associated with lower self-reported burnout and reduced after-hours documentation time.58 Another recent study involving five academic centers shows AI scribe adoption associated with decreases in EHR and documentation time—and an increase in time for patient visits, with benefits for both primary care physicians and advanced practice clinicians.59 Redesigning care Expanding effective capacity requires redesigning care delivery, not simply adding personnel. Technology can support that redesign when it shifts routine work across the care team, supports delegation, and enables clinicians to practice at the top of their license. The National Academies’ framework for high-quality primary care emphasizes that interoperable data systems and shared infrastructure are essential for effective teams.60 Without them, clinicians must often spend time on routine tasks, limiting time with patients and contributing to burnout.61 Clinical decision support tools and shared dashboards can permit supervising clinicians to focus on exceptions rather than duplicating routine work. In areas such as documentation, prior authorization, and inbox management, workflow redesign supported by automation can enhance time for direct patient care. But technology should support decision making, not replace it: FDA guidance on clinical decision support software likewise emphasizes that clinicians must be able to independently review the basis for recommendations.62 Here, again, technology’s role will grow: Gawin believes that AI can help “demystify” challenging cases by providing better data for decision making in individual cases, allowing practitioners to focus more intently on the patient and making teams “smarter and more confident.” Adoption of new technology should be tied to clear operational needs, supporting workflow, and governance frameworks that preserve human oversight, transparency, and accountability. Tools are more likely to improve capacity when organizations pair them with workflow redesign, training, and clear operational use cases rather than layering them onto existing routines and expecting adoption to happen on its own. Prevention and screening Technology-enabled prevention and screening can reduce pressure on clinics and hospitals by shifting monitoring and early intervention into settings such as the home, pharmacies, and remote channels. This may be especially important in long-term care, home-based care, and other settings even as staffing remains constrained. A 2025 systematic review and meta-analysis found that remote patient monitoring could reduce hospitalization and shorten lengths of stay, though effects varied by population and implementation.63 Related models that combine remote monitoring with structured clinical pathways extend the same logic into higher-acuity care. A 2024 cohort study similarly found that an acute virtual home-care model with remote monitoring was associated with shorter hospital stays without significant increases in mortality or return utilization.64 Preventive management programs show similar potential in chronic disease: one clinical trial found that home blood pressure telemonitoring combined with pharmacist management improved blood pressure control. However, these beneficial results remain highly dependent on program design and workflow integration.65 Risk and governance As digital tools become more prominent in care delivery, governance increasingly shapes not only safety and liability, but also the clinician-patient relationship. Decision support systems can introduce safety, bias, and liability concerns if guardrails are unclear, and algorithms that influence triage, utilization, or care pathways can shape clinical and financial decisions. Sustaining workforce trust and public confidence therefore requires transparency and preserving clinician accountability. Michael Betz, Chief Growth & Innovation Officer and President of Walden University, notes that AI is less a technology challenge than a change management challenge and that real adoption starts with the people closest to the work.66 As AI tools evolve, organizations will need continuing education, clearer governance, and stronger digital fluency among clinicians, staff, and patients if technology is to expand capacity and truly be complementary to human clinicians without weakening confidence or safety. Aligning payment with technology-enabled care models Technology adoption will remain limited, however, if payment policy does not support the settings and workflows where digital tools generate value. Coverage and reimbursement decisions therefore shape whether remote monitoring, telehealth, and team-based digital become durable components of workforce strategy and thus the pace of innovation. CMS’ telehealth policies show real progress in moving some remote services into more routine reimbursement, including permanent additions to the Medicare telehealth services list and continued payment flexibility for certain settings and services, but they also illustrate how viability can still depend on service-specific billing rules and time-limited extensions.67 The Accountable Care Organization Primary Care Flex model addresses a different constraint: it tests whether prospective primary care payments give organizations the financial stability to invest in staffing, coordination, and more proactive team-based care that fee-for-service often fails to support.68 Together, these initiatives underscore that new care models are far more likely to endure when payment rules support the staffing, coordination, and infrastructure they require rather than reimbursing only episodic encounters. The path forward will depend on whether policymakers can align training capacity, job quality, payment design, regulatory flexibility, and technology adoption around modern models of care. Shortages will persist if the system continues to underinvest in entry pathways, rely on administrative workarounds to sustain delivery, and reward fragmented care more readily than prevention, coordination, and team-based practice. Other factors in the health care system, for instance the role of both public and private insurers, also affect workforce capacity. For many of the solutions discussed above, the role of employers in fostering an environment for success is clear. But there is a broader role for employers as well: to foster a culture that supports workforce training, retention, career growth, and better health outcomes. Most basically, this is a mindset that focuses intentionally and intensely on the skill and compassion of employees. At Northwell Health, this involves deep personal commitment; the CEO meets every new employee personally as a critical step in workforce development. Speaking to new employees, he emphasizes the uniqueness of health care as a profession—the demands of the position, the need for compassion in all that employees do in caring for patients and their families, the importance of soft skills and relationships in addition to technical excellence—and both challenges them and underscores the importance of their role in building a culture of excellence in care. This effort to close the gap between the CEO and frontline workers helps top management connect to the concerns of frontline workers and serves as a catalyst to build the organization’s culture, strengthening retention by ensuring that from the outset of their employment, workers understand both the organization’s expectations and their value to the organization, so that they can be proud of all the organization does to care for people. In short, business plays an indispensable role here: as Steve Beard of Covista notes, one starting point is a “passion for getting more people into health care careers and giving them a future.”69 Facing these challenges will require innovative leaders to address workforce shortages and move the industry forward to serve an aging population in which demand for health care services of all types will be strong. Systemic change, regulatory change, policy change, and business leadership are all necessary to meet the challenge. This Solutions Brief has outlined a number of challenges and headwinds the industry faces and offered steps towards real solutions. It is equally important to note the tailwinds, those positive forces that characterize the health care workforce every day: resilience, grit, optimism, innovation, and leadership. The Nation felt this during the COVID-19 pandemic, seeing health care workers at all levels afresh, and as the heroes they are. In addressing today’s health care workforce challenges, it will be essential to recover the sense of urgency that characterized the pandemic to find and implement innovative solutions now while focusing on education and training for the workers who will be the durable solution to our current workforce shortages, and who will work in a health care system with routine use of advanced technology. As during the pandemic, business leaders must participate directly in this search for solutions to a national challenge. Covista, Covista Care Capacity Monitor , 2026; Steve Beard, remarks at the Health Care Workforce Policy Summit, Committee for Economic Development of The Conference Board, New York, NY, March 25, 2026. Although the summit was held under the Chatham House Rule, Mr. Beard agreed to have his comments used publicly in this report. Organisation for Economic Co-operation and Development, Health at a Glance 2025 , Paris 2025. Committee for Economic Development of The Conference Board, Health Care Workforce Policy Summit: Insight Summary , The Conference Board, March 30, 2023. US Bureau of Labor Statistics, Current Employment Statistics—CES (National): Table B-1a. Employees on Nonfarm Payrolls by Industry Sector and Selected Industry Detail, Seasonally Adjusted dashboard, US Department of Labor, 2026. Lydia DePillis, Health Care Hiring Labor Market , New York Times, March 6, 2026. Steve Beard, remarks at the Health Care Workforce Policy Summit, Committee for Economic Development of The Conference Board, New York, NY, March 25, 2026. Although the summit was held under the Chatham House Rule, Mr. Beard agreed to have his comments used publicly in this report. Bureau of Health Workforce, Health Resources and Services Administration, Health Workforce Projections , December 2025. Bureau of Health Workforce, Health Resources and Services Administration, How We Define Rural , September 2025. Covista, Covista Care Capacity Monitor , 2026. US Census Bureau, Older Population Grew Faster Than Younger Population From 2010 to 2020 , May 25, 2023. Federal Interagency Forum on Aging Related Statistics, Older Americans 2024: Key Indicators of Well-Being , May 2024. Steve Beard: “There is no shortage of talent; there is a shortage of opportunity.” American Association of Colleges of Nursing, Nursing Faculty Shortage Fact Sheet , February 2026. American Hospital Association News, Medical School Enrollment Hits New Record , January 10, 2025. Government Accountability Office, Caps on Medicare-Funded Graduate Medical Education at Teaching Hospitals, 2021. National Resident Matching Program, NRMP Releases 2025 Main Residency Match Results and Data Report, Providing In-Depth Insight into the Largest Residency Match in History , May 29, 2025. Michael J. Dowling, remarks at the Health Care Workforce Policy Summit, Committee for Economic Development of The Conference Board, New York, NY, March 25, 2026. Although the summit was held under the Chatham House Rule, Mr. Dowling agreed to have his comments used publicly in this report. Steve Beard, remarks at the Health Care Workforce Policy Summit, Committee for Economic Development of The Conference Board, New York, NY, March 25, 2026. Although the summit was held under the Chatham House Rule, Mr. Beard agreed to have his comments used publicly in this report. Joseph Kemp, Northwell School of Health Sciences Opens in Queens , Northwell News, September 2, 2025. ApprenticeshipUSA, Healthcare , US Department of Labor, and Health Care Apprenticeship Consortium, About Us . Association of American Medical Colleges, Medical Student Education: Debt, Costs, and Loan Repayment Fact Card for the Class of 2024 , October 2024. Covista, Chamberlain University and SSM Health Launch Landmark Partnership to Address Nursing Shortage , July 9, 2025. Covista, Our Impact , February 2026. Northwell Health, Quality: 2017 Clinical Excellence and Quality Annual Report , 2017. Health Resources and Services Administration, Bureau of Health Workforce, Teaching Health Center Graduate Medical Education (THCGME): Expanding the Primary Care Workforce , June 2026. Mary Ellen Gabriel, Training Doctors for Rural Practice Helps Meet Statewide Need , School of Medicine and Public Health, University of Wisconsin, April 25, 2024. Howard K. Rabinowitz, Robert J. Motley, Fred W. Markham Jr., and Gillian A. Love, Physician Shortage Area Program and Lessons Learned as Thomas Jefferson University's Rural Physician Shortage Area Program (PSAP) Approaches the Half-Century Mark , Thomas Jefferson University Academy of Medicine, September 1, 2022. The Conference Board, Modernizing Health Programs for Fiscal Sustainability and Quality webcast, aired November 18, 2024. The Conference Board, Navigating the Health Care Landscape in 2026 , December 1, 2025. Shishir Shakya, Understanding the Role of Immigrants in US Health Sector Employment , Baker Institute for Public Policy, January 3, 2024.? Association of American Medical Colleges, 2025 Key Findings and Definitions , 2025. Raed Hailat, Mohamed Ridha, Chun Chieh Lin, Kevin Kerber, and James F. Burke, Trends in the Proportion of US and International Medical Graduates at the County Level , National Library of Medicine, August 14, 2025. Drishti Pillai, Matthew Rae, and Samantha Artiga, The Growing Role of Foreign-Educated Nurses in US Hospitals and Implications of Visa Restrictions , KFF, July 10, 2024. Priya Chidambaram and Drishti Pillai, What Role Do Immigrants Play in the Direct Long-Term Care Workforce?, KFF, April 2, 2025. Breno Braga et al., Migration Policy and the Supply of Foreign Physicians: Evidence from the Conrad 30 Waiver Program , National Bureau of Economic Research Working Paper No. 32005, December 2023. The Conference Board, Addressing Shortages in the Health Care Workforce: Insights and Solutions from the Committee for Economic Development Healthcare Business Roundtable , January 25, 2023. Committee for Economic Development, Addressing Shortages in the Health Care Workforce , January 2023. Cleveland Clinic, Flexible Scheduling Helps Attract and Retain Nurses , March 10, 2023. Committee for Economic Development, Addressing Shortages in the Health Care Workforce, January 2023. Northwell Health, Center for Learning and Innovation . Angela C. Keith, Nora Warshawsky, and Steve Talbert, Factors That Influence Millennial Generation Nurses' Intention to Stay: An Integrated Literature Review . The Journal of Nursing Administration 51, No. 4 (April 2021): 220-226. Agency for Healthcare Research and Quality, TeamSTEPPS Program . Pamela Mitchell, Matthew Wynia, Robyn Golden, Bob McNellis, Sally Okun, C. Edwin Webb, Valerie Rorhbach, and Isabelle Von Kohorn, Core Principles & Values of Effective Team-Based Health Care , Institute of Medicine of the National Academies, October 2012. Bianca Frogner, How Do You Create a ‘Zero-Burnout’ Primary Care Practice? , Tradeoffs, July 2, 2021. Committee for Economic Development, Addressing Shortages in the Health Care Workforce, January 2023. Office of the Law Revision Counsel, 42 U.S.C. 138-95nn, June 16, 2026. Rachel Reid, Cheryl Damberg, and Mark W. Friedberg, Primary Care Spending in the Fee-for-Service Medicare Population , JAMA Internal Medicine 179, Vol. 179,7 No. 7 (April 2019): 977-980. Zirui Song, Paying Primary Care More—Will It Work This Time? , JAMA Internal Medicine 334, No. 18 (September 2025): 1617-1618. Corinne Lewis, Celli Horstman, and Alexandra Bryan, How Upfront, Predictable Payments Can Improve Primary Care , To the Point Blog, May 13, 2024. National Conference of State Legislatures, Nurse Practitioner Scope of Practice and Prescriptive Authority . National Academy for State Health Policy and Milbank Memorial Fund, Implementing High-Quality Primary Care: A Policy Menu for States , September 2, 2025. Interstate Medical Licensure Compact Commission, Interstate Medical Licensure Compact Commission Annual Report FY2025 , January 2026. National Council of State Boards of Nursing, Nurse Licensure Compact Annual Report Fiscal Year 2024 , 2025. Health Resources and Services Administration, Licensure Portability Grant Program , February 2024. US Department of Health and Human Services Centers for Medicare & Medicaid Services, Advancing Rural Health Equity: Fiscal Year 2022 Year in Review , November 2022. US Department of Health and Human Services Centers for Medicare & Medicaid Services, Medicare Telehealth Trends, 2025. Committee for Economic Development of The Conference Board, Health Care Policy After the Pandemic , The Conference Board, October 30, 2023. Kristine D. Olson, Daniella Meeker, Matt Troup, et al., Use of Ambient AI Scribes to Reduce Administrative Burden and Professional Burnout , JAMA Network Open 8, No. 10 (October 2024) Lisa S. Rotenstein, A. Jay Holmgren, and Robert Thombley et al., Changes in Clinician Time Expenditure and Visit Quantity With Adoption of Artificial Intelligence–Powered Scribes: A Multisite Study , JAMA 335, No. 16 (April 2026): 1408-1417. National Academies of Sciences, Implementing High-Quality Primary Care: Rebuilding the Foundation of Health Care, National Academies of Sciences, Engineering, and Medicine , 2021. A. Jay Holmgren, Nathaniel Hendrix, Natalya Maisel et al., Electronic Health Record Usability, Satisfaction, and Burnout for Family Physicians , JAMA Network Open 7, No. 8 (August 2024) US Food and Drug Administration, Clinical Decision Support Software: Guidance for Industry and Food and Drug Administration Staff , January 2026. Geir Smedslund, Nina Østerås, and Christine Hillestad Hestevik, Effects of Remote Patient Monitoring on Health Care Utilization in Patients With Noncommunicable Diseases: Systematic Review and Meta-Analysis , JMIR mHealth and uHealth, October 2025. Josh Banerjee, Christopher Lynch, Hugh Gordon et al., Virtual Home Care for Patients With Acute Illness ,JAMA Network Open 7, No. 11 (November 2024) Monica L. Taylor, Emma E. Thomas, Centaine L. Snoswell, Anthony C. Smith, Liam J. Caffrey et al., Does Remote Patient Monitoring Reduce Acute Care Use? A Systematic Review , BMJ Open 11, No. 3 (March 2021). Steve Beard, The Healthcare Workforce Crisis is Real and It’s Happening Now , LinkedIn, April 2026. Centers for Medicare & Medicaid Services, Telehealth , February 9, 2026. Centers for Medicare & Medicaid Services, Telehealth FAQ , February 26, 2026, Steve Beard, The Healthcare Workforce Crisis is Real and It’s Happening Now , LinkedIn, April 2026.
Trusted Insights for What’s Ahead®
Recommendations
Understanding the Workforce Gap
Mapping Current and Future Shortages
Why Health Care Shortages Persist
Practical Solutions for the US Health Care Workforce
Considering all of this, one essential task is to encourage more students to pursue primary care—for most people, the gateway to the health system. This includes not only physicians specializing in primary care but also ensuring sufficient supply of other gateway access points to the system, such as nurse practitioners, physician assistants, and the infrastructure that supports these efforts. This will not only help solve critical shortages but improve health outcomes, given that stronger primary care is essential to prevention, care coordination, improved outcomes, and long-term cost control.28 29Immigration policy
Older and independent workers
Scope of practice and licensure
Technology and AI: Amplifying the Workforce
Employers’ Role: Strengthening the Health Care Workforce for the Future
Endnotes
Solutions to the US Health Care Workforce Shortages
June 25, 2026
A Bipartisan Fiscal Commission to Tackle the National Debt
February 17, 2026
250 Years Forward
January 20, 2026
